
Surgery removes the tumor. But the days around the operation are when cancer can quietly spread and seed a return. Dr. Paul Marik’s updated guide gives clinicians a practical, low-risk plan to protect that window.

For most patients with a solid tumor, surgery is the definitive step: remove the cancer, recover, move on.
What’s rarely explained is that surgery itself can change the biology of cancer. It can spill tumor cells into the bloodstream. It can lower immune defenses at the moment they’re needed most. And it can set the stage for a recurrence that surfaces years later.
Patients are often told a recurrence is just something that “may happen.” But the perioperative window is a moment where smart, low-risk steps may tip the odds the other way.
IMA Chief Scientific Officer Dr. Paul Marik built this guide to do exactly that. It’s a practical companion to his Cancer Care monograph, written for the oncologist or integrative physician on the patient’s team, and for the patient who wants to bring it to them.
“Almost anyone who is going to have a surgical intervention to remove a cancer should consider this therapy, and the protocol is outlined in our guidance.” — Dr. Paul Marik
📘 About This Guide
This guide was authored by Dr. Paul Marik, IMA Chief Scientific Officer, to translate the science behind perioperative interventions into action a clinician can use.
It’s one of a growing library of focused companion guides to the Cancer Care monograph. Related companions include:
- The Approach to Repurposed Drugs for Cancer
- Targeting Cancer Stem Cells
- Stopping the 10 Deadliest Cancers
The full monograph carries the detailed evidence and references. This guide delivers immediate insight into a critical, often overlooked step in cancer care. As the guide itself notes, care should be supervised by an integrative clinician; this is not a protocol for patients to run on their own.
🧬 Why Surgery Can Accelerate Metastasis
Surgery is the right step for most solid tumors. The problem is what the operation does to the surrounding biology in the process. Removing a tumor disrupts the tissue and blood vessels around it, which can spill cancer cells into the bloodstream or seed them into the chest or abdominal cavity.
At the same time, surgery sets off a chain of signals that work in the cancer’s favor:
- Cancer cells spill into the blood or lymphatic system as the tumor is disturbed.
- Inflammatory cytokines surge (interleukin-1 and interleukin-6) in the body’s normal response to a wound.
- Immune defenses drop at the exact moment they’re most needed.
- COX-2 activity spikes, an inflammatory enzyme that fuels new blood vessel growth and helps circulating cancer cells stick to vessel walls.
Together these create conditions where a circulating tumor cell is far more likely to stick, survive, and settle somewhere new. Researchers call this sequence the metastatic cascade.
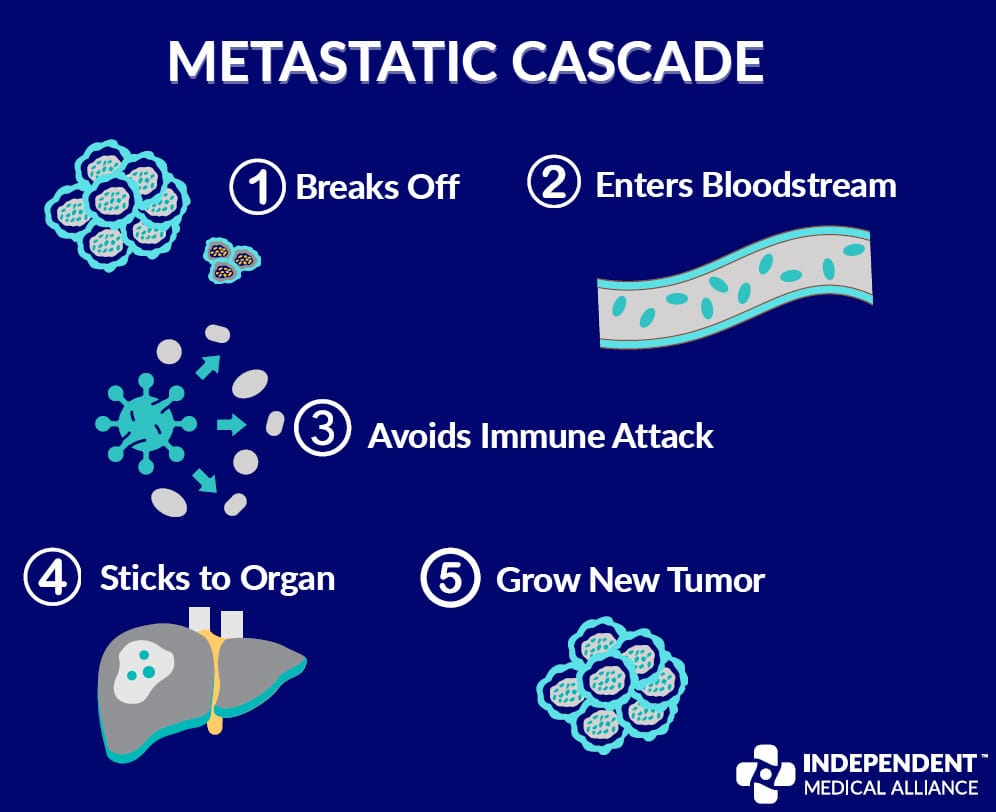
⚠️ The bottom line: the cascade speeds up when inflammation is high and immune defenses are low, exactly the state surgery creates. That window is biologically dangerous, but it’s also medically addressable.
⏳ Why Recurrence Can Surface Years Later
A recurrence isn’t random, and it isn’t always quick. A cancer cell that survives the journey has to multiply to roughly a billion cells before it’s even detectable on a scan, about 30 doublings. Depending on the tumor, a single doubling can take anywhere from weeks to years.
That math explains something patients are rarely told: metastases from a slow-growing tumor can stay invisible for a decade after a “successful” operation.
The guide points to a striking example. In an analysis of women with breast cancer, surgery clearly improved early survival, but the data showed a spike in mortality around year eight in the surgery group, a pattern not seen in those who didn’t have surgery. The takeaway isn’t that surgery is the wrong choice. It’s that the perioperative window deserves a deliberate plan to counter each mechanism surgery sets in motion.
💊 The Four-Drug Perioperative Protocol
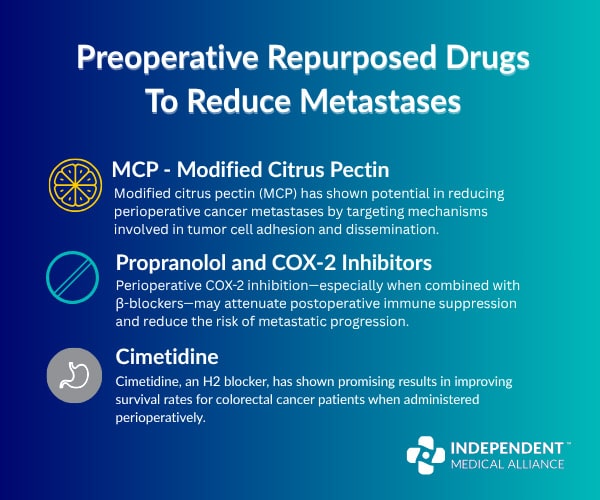
The guide focuses on four repurposed medications, all inexpensive, widely available, and well-characterized. Each targets a different way surgery helps cancer spread.
✅ Modified Citrus Pectin (MCP)
- Blocks galectin-3, the adhesion molecule cancer cells use to clump together and latch onto blood vessel walls.
- In lab and animal studies, reduced metastasis by 40 to 90%, and inhibited cancer cell adhesion and invasion by up to 95% in vitro.
- Safe, non-toxic, and taken orally. Human trials are still needed to confirm the perioperative benefit.
✅ Propranolol (beta-blocker)
- Dampens the stress-adrenaline signaling that drives cancer spread, and improves immune cell infiltration into tumors.
- A 2025 systematic review of 31 studies found propranolol may improve outcomes, especially when given around the time of surgery.
- Works best paired with a COX-2 inhibitor.
✅ COX-2 Inhibitors (e.g., ketorolac, etodolac)
- Blunt the post-surgical inflammatory surge that helps cancer cells take hold.
- In the COMPIT trial, perioperative propranolol plus a COX-2 inhibitor cut 5-year recurrence in colorectal cancer patients from 50% to 12.5%.
- Selective COX-2 inhibitors don’t raise perioperative bleeding risk, but should be reserved for patients with a favorable cardiovascular profile.
✅ Cimetidine (H2 blocker)
- Prevents tumor cells from attaching to blood vessel walls by suppressing E-selectin.
- In colorectal cancer, improved 10-year survival from 49.8% to 84.6%.
- A benefit unique to cimetidine; other H2 blockers like famotidine and ranitidine don’t show the same effect.
📋 Suggested Perioperative Protocol
| Drug | Dose | Timing |
|---|---|---|
| MCP | 10–15 g/day (divided) | 5 days before → 6–12 months after |
| Propranolol | 40–80 mg BID | Start 5 days pre-op, taper 2–4 weeks post-op |
| COX-2 Inhibitor | Per clinician judgment | Around the day of surgery |
| Cimetidine (colorectal) | 800 mg/day | 5 days before → 1 year after |
Two practical notes from the guide: cimetidine raises propranolol blood levels, so the propranolol dose needs adjusting when both are used, and the anesthesiologist should be told the patient is on a beta-blocker.
🌟 Turning Risk Into Opportunity
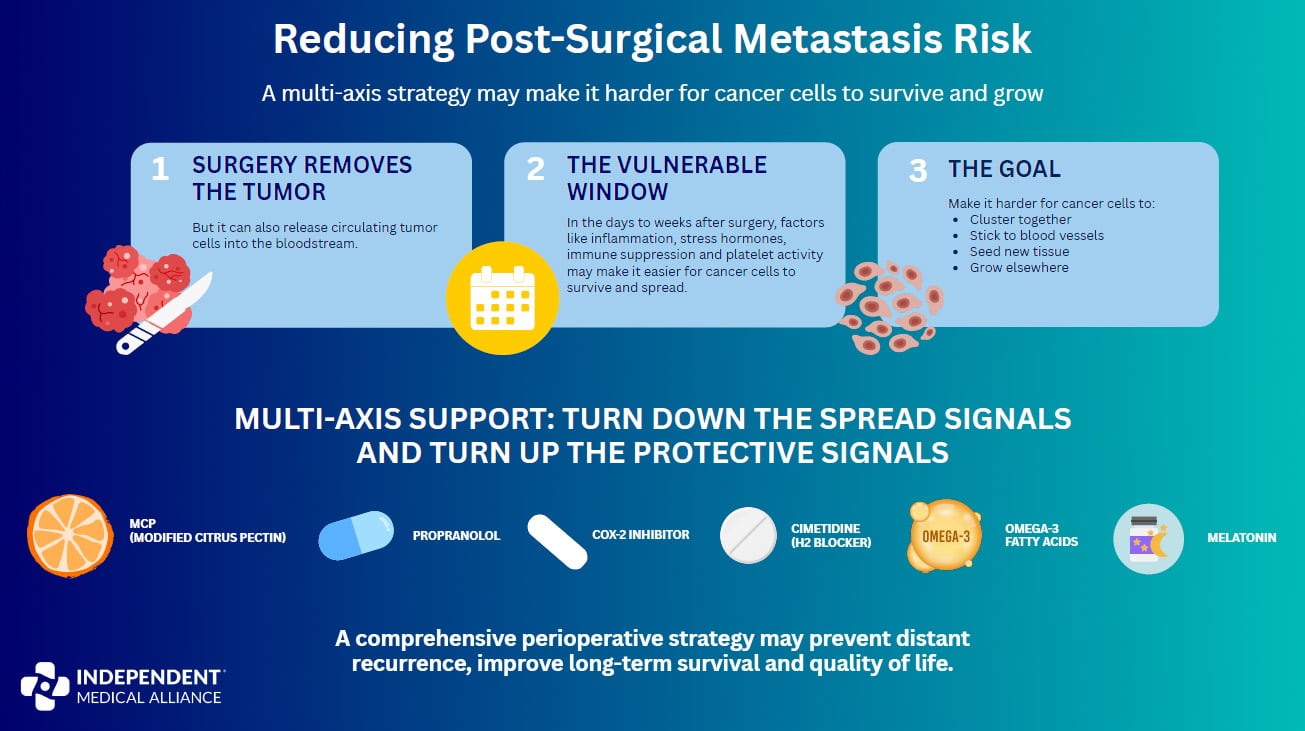
Surgery doesn’t just remove cancer. It opens a window. That window can leave a patient vulnerable, or, with the right plan, it can become a point of protection.
The four-drug protocol is the core, but the guide notes it fits naturally alongside other metabolic strategies IMA covers elsewhere, including omega-3 fatty acids, melatonin, vitamin D, and perioperative fasting. (That’s why you’ll see a few of them in the summary graphic below.)
This is a message both patients and providers deserve to hear. The summary infographic below is built to share.
📚 More Cancer Care Resources
- Monograph: Cancer Care
- Hub: IMA Cancer Resource Hub
- Guide: The Approach to Repurposed Drugs for Cancer
- Guide: Cancer Resistance
- Guide: The Metabolic Trap
- Guide: Dietary Interventions in Cancer
- Guide: Cancer Nutrition Guide

