
A new review by IMA researchers shows that most new cancer drugs help fewer than 2% of patients, and makes the case for the cheaper, broader strategies the system keeps ignoring.

The world spends roughly $550 billion on cancer every year. And yet the drugs coming out of that investment keep reaching fewer people, not more.
Of the 14 new cancer drugs the FDA approved in 2024, 10 are indicated for less than 2% of all cancers. For the millions of patients and families facing a diagnosis every year, the pipeline that is supposed to help them is getting narrower, not wider.
Cancer is the second leading cause of death in the United States, and most of what drives it is preventable: diet, chemical exposures, physical activity, sleep. The treatments that could address it broadly already exist. They are cheaper, more widely applicable, and backed by growing evidence.
A new review by IMA researchers charts a different course. Published in Annals of Research in Oncology by IMA researchers Matthew Halma, Dr. Paul Marik, Dr. Joseph Varon, and collaborator Jack Tuszynski, it makes the case that the tools are already here. The system just has not been pointed at them.
📖 Read the Full Paper
Beyond Targeted Therapy: Environmental Determinants and Metabolic Strategies in Cancer Prevention and Treatment (Annals of Research in Oncology, 2026) — Authors: Matthew Halma, Paul Marik, Joseph Varon and Jack Tuszynski

The Narrow Pipeline
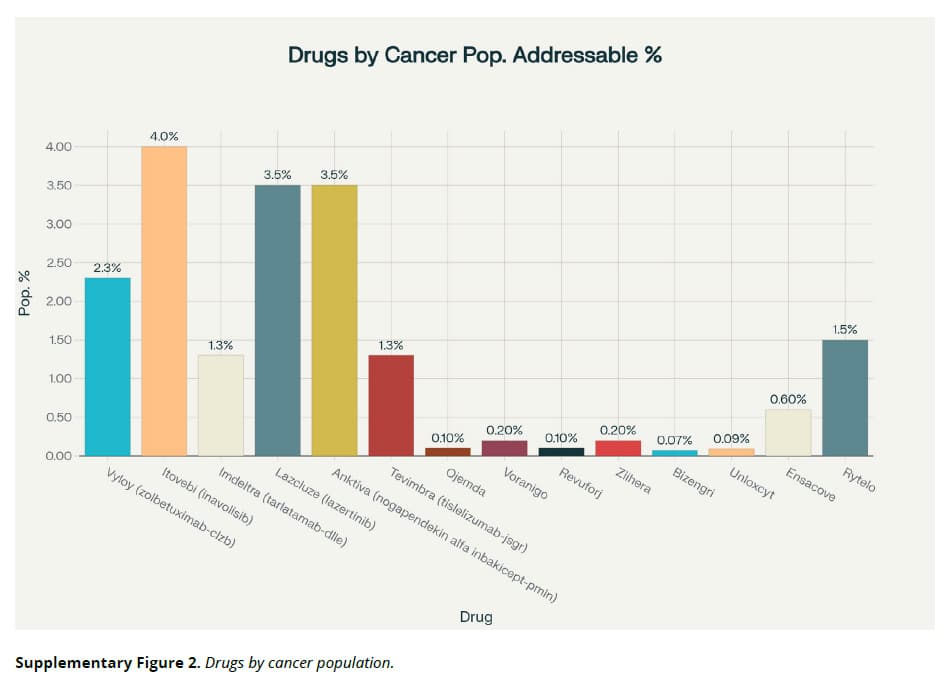
The review includes a table that puts the problem in plain terms. For every new cancer drug approved in 2024, the authors calculated what percentage of cancer patients it could actually help.
- Itovebi (a specific type of breast cancer): ~4% of all cancers
- Lazcluze (a specific type of lung cancer): ~3.5%
- Imdeltra (small cell lung cancer): ~1.3%
- Ojemda (a rare childhood brain tumor): ~0.1%
- Bizengri (an extremely rare lung/pancreatic mutation): ~0.07%
These drugs represent real advances for specific patients. But the pattern is hard to miss: billions of dollars flowing into treatments that serve narrow slices of the disease, while the strategies that could reach far more people sit on the margins.
What’s Driving Cancer
Another major theme the review explores is what is actually driving cancer. And while the pipeline is narrowing, the causes are not. The list is long, but three major threads stand out.
The food system is working against us.
- Heavily processed foods are linked to higher cancer risk through multiple pathways: too many calories, too few nutrients, additives that damage the gut, and a microbiome that is increasingly disrupted
- Dietary nutrient density per calorie is inversely associated with cancer risk
- Glyphosate use increased nearly 15-fold between 1994 and 2014, from 56,000 to 825,000 tons
Everyday exposures add up.
- Radon gas is the second leading cause of lung cancer after smoking, and it accumulates indoors
- Flame retardants in furniture are associated with more than double the risk of thyroid cancer
- Air pollution drives hundreds of thousands of lung cancer cases worldwide each year
Lifestyle factors compound the damage.
- Physical inactivity: two-thirds of adults do not meet basic physical activity guidelines
- Sleep deprivation: more than a third sleep fewer than seven hours a night
- Antibiotic exposure is associated with a 37% increased cancer risk between the lowest and highest exposure groups
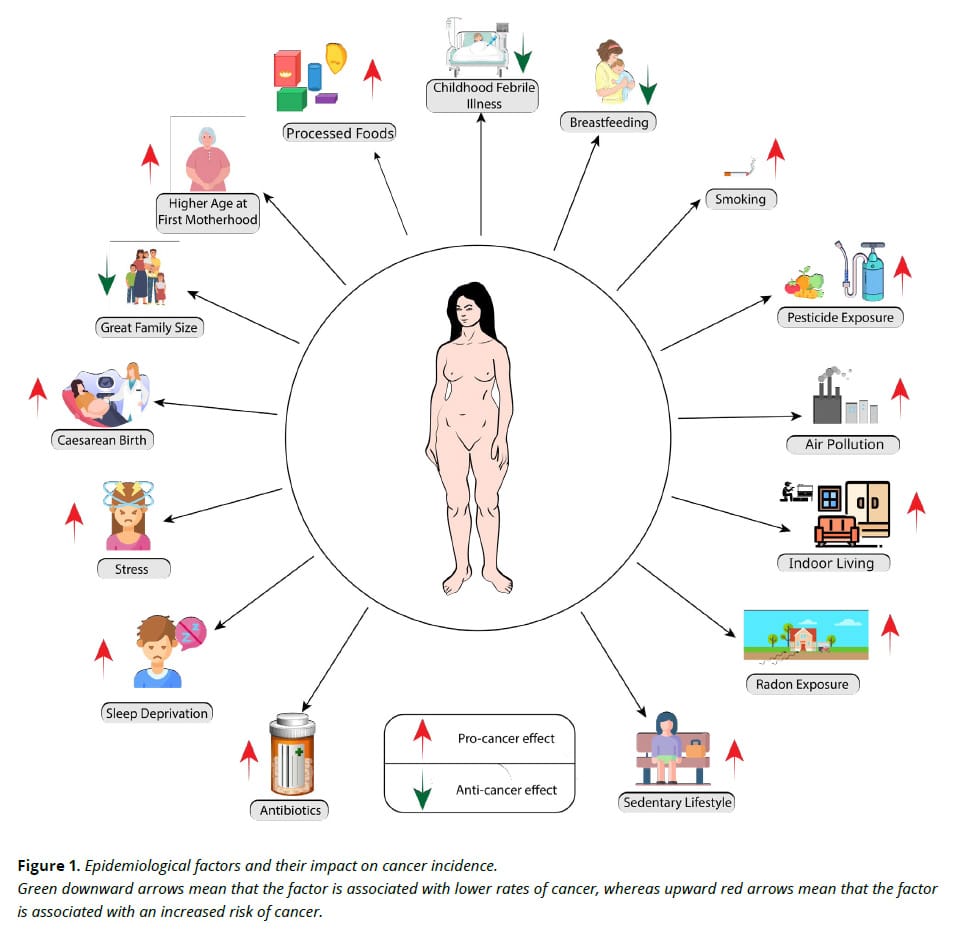
These factors do not act alone. They accumulate, and most of them are preventable.
Broader Treatments Already Exist
New cancer drugs cost over a billion dollars to develop, take nearly eight years to reach patients, and safety problems can go unaddressed for years after approval. Repurposed drugs skip most of that. The paper identifies three treatment areas that could reach far more patients at a fraction of the cost:
- Repurposed drugs: known safety profiles built on decades of real-world use, generic pricing, established manufacturing, and computational tools that are accelerating the discovery of new anti-cancer applications
- Dietary and metabolic strategies: with 40–80% of cancer patients experiencing malnutrition, nutrition is a clinical priority. There are currently 53 clinical trials testing ketogenic diets in cancer on clinicaltrials.gov, with several already showing survival improvements
- Multidrug combinations: using multiple repurposed drugs to attack cancer through several pathways at once, making resistance harder to develop
The evidence base for each of these is at different stages, and the authors are careful to note that novel drug combinations carry risk and should be introduced gradually. But the direction is clear: broadly applicable, lower-cost strategies deserve investment proportional to their potential.
IMA has been building the case for these strategies for years:
Built on Cancer Care
Those resources did not appear out of thin air. IMA’s cancer work started with Dr. Paul Marik’s Cancer Care monograph, which established the framework for metabolic therapy and repurposed drugs. It remains IMA’s most widely read cancer resource. This review extends that foundation into environmental prevention and integrative care.
Many IMA doctors already work as integrative oncologists, and the demand is only growing. A majority of US cancer patients use some form of complementary medicine during treatment. Nearly half never tell their oncologists, because they already know what the answer will be.
More and more guidelines support integrative approaches, even the ones written by mainstream oncology. The evidence supports them. The patients want them. Yet most oncologists still will not engage, not because the evidence is missing, but because the training is. That is the gap IMA was built to fill, and the Cancer Resource Hub is where all of that work comes together.
Related Reading
- Monograph: Cancer Care: Repurposed Drugs & Metabolic Interventions
- Hub: Cancer Resource Hub
- Post: Our Approach: Repurposed Drugs for Cancer
- Post: The Metabolic Trap: Targeting Five Cancer Pathways at Once
- Post: Dietary Interventions in Cancer: Targeting Tumor Metabolism Through Diet
- Post: Drug Cycling in Cancer Care: What It Is and Why It’s Critical

More on: cancer | Dr. Joseph Varon | Dr. Paul Marik | Matthew Halma | Medical Journals | Medical Research
