
Host: Dr. Ryan Cole | Guest: Dr. Paul Marik
What happens when a cancer treatment stops working the way it once did? In many cases, knowing when and how to change therapies may be just as important as the treatment itself.
This week, host Dr. Ryan Cole, IMA Head of Medical & Scientific Affairs, is joined by Dr. Paul Marik, IMA Chief Scientific Officer, for a timely conversation on the role of drug cycling in cancer care and why it may be essential to improving outcomes for patients.
Cancer treatment is evolving. Thanks to the work of researchers like Dr. Paul Marik, a growing body of evidence shows that repurposed drugs and metabolic strategies can punch far above their weight class, often outperforming the outcomes patients see from chemotherapy and radiation alone. Patients and providers around the world are reporting real results.
But with that progress comes a new challenge. A physician recently reached out to Dr. Marik with a troubling pattern: his patients would respond well to metabolic therapy for the first two years, and then their tumors would spiral out of control. Nothing he tried could get them to respond again. That question sent Dr. Marik down a research path that led to a surprising discovery—simple, powerful concepts that had never been highlighted in the published literature. Those findings led to the creation of two brand-new Cancer Care companion guides, both of which are explored in this week’s conversation.
Meet the Experts

Dr. Paul Marik
IMA Chief Scientific Officer. Author of Cancer Care. Dr. Marik is one of the most published critical care physicians in the world, with over 500 peer-reviewed publications. His ongoing research into repurposed drugs and metabolic approaches to cancer has produced a growing body of freely available clinical guides for patients and practitioners through IMA’s Cancer Resource Hub.

Dr. Ryan Cole
IMA Head of Medical & Scientific Affairs. Board-certified pathologist. Dr. Cole brings decades of experience in cancer diagnostics and a cell-level understanding of how tumors behave, adapt, and resist treatment. His expertise in tissue pathology gives him a unique vantage point on why cancers respond to some therapies and evade others.
1. New Cancer Care Guides: Why They Matter
IMA’s metabolic approach to cancer is built on Cancer Care, Dr. Marik’s comprehensive monograph on repurposed drugs and nutraceuticals in cancer treatment. Cancer Care is a living body of work, supported by companion guides that get updated as new evidence emerges. The companion guide on repurposed drugs alone is now on its 26th version. As Dr. Marik notes, that’s the advantage of publishing online rather than in print: “A book is static. It doesn’t grow and it’s usually outdated very quickly.”
Cancer Care is supported by a growing library of companion guides, each focusing on a specific aspect of the metabolic approach. This week, IMA is releasing two new additions:
The Metabolic Trap
A new framework for simultaneously targeting five metabolic pathways in the cancer cell.
Cancer Resistance
What to do when a metabolic protocol stops working, and how to prevent it from happening in the first place.
This week’s conversation introduces the thinking behind both guides.
2. The Hidden Detail That Changes Everything
There’s a four-drug regimen for glioblastoma called the METRICS protocol. It combines atorvastatin, metformin, doxycycline, and mebendazole, and it’s well known among naturopathic and integrative oncologists.
What almost nobody knows is that the paper associated with the protocol left out a critical detail.
Buried in the original, unpublished version was a specific instruction: cycle the doxycycline and mebendazole one month on, one month off. The researchers did this deliberately, but never highlighted it in their published findings. As Dr. Marik explains, that cycling was the mechanism that prevented resistance.
“If you have constant pressure on that pathway, just by evolutionary biology, the cells will adapt and mutate, so they become resistant.” — Dr. Paul Marik
Drugs like doxycycline and mebendazole each target a single metabolic pathway in the cancer cell. Sustained, unrelieved pressure on one pathway gives the cell time to evolve around the blockade. Once resistance develops on one pathway, it can cascade into multi-drug resistance.
Drugs that act on multiple pathways simultaneously, like curcumin and metformin, are less prone to this problem. But for single-pathway agents, cycling is what keeps the cancer from adapting.
For patients who have watched a promising treatment lose its effectiveness, this is meaningful. It means what happened wasn’t random, and there are strategies to address it.
3. Multi-Axis Metabolic Pressure: Targeting Five Pathways at Once
From that insight, Dr. Marik developed what he calls Multi-Axis Metabolic Pressure. The concept is to simultaneously block five metabolic pathways in the cancer cell so it has no remaining source of energy.
The five axes and their corresponding agents:
- Warburg effect (glucose dependence): Metformin + berberine
- Mitochondrial function: Doxycycline
- Cytoskeleton: Mebendazole
- Adrenergic signaling: Propranolol
- Oxidative stress and circadian rhythm: Melatonin
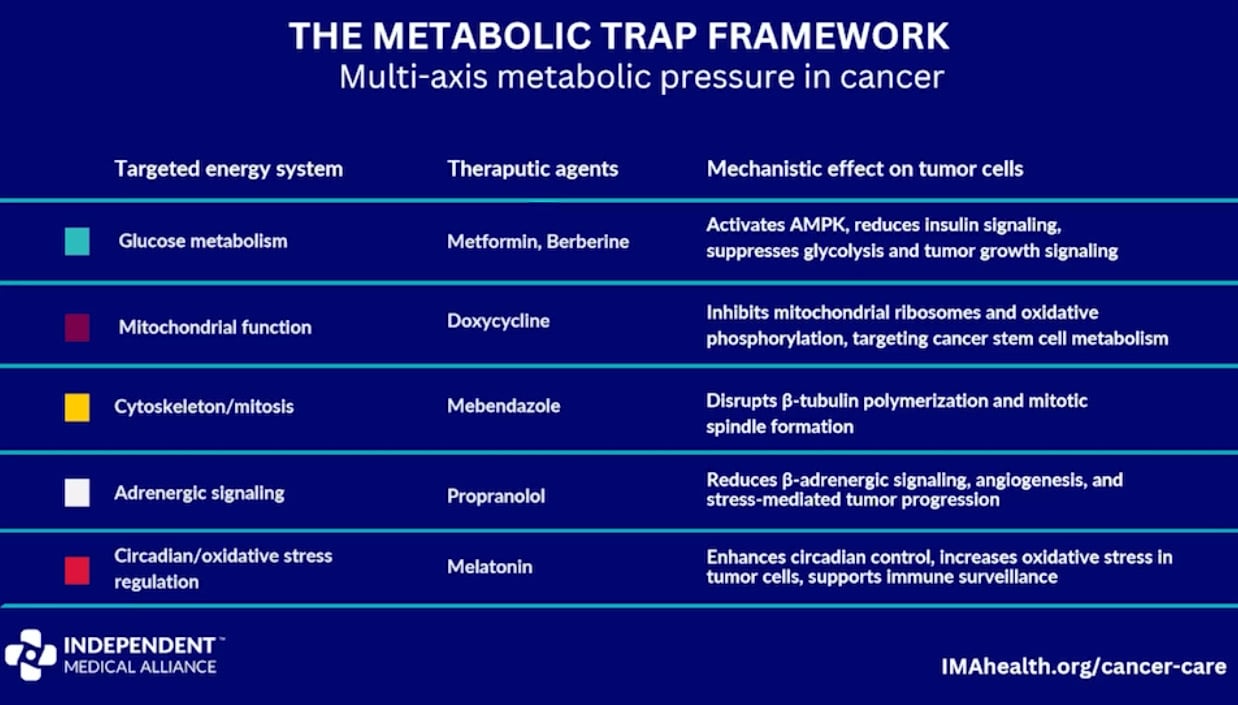
“With these five used in combination, you completely whack-a-mole the cancer cell. It has no way of getting energy and surviving.” — Dr. Paul Marik
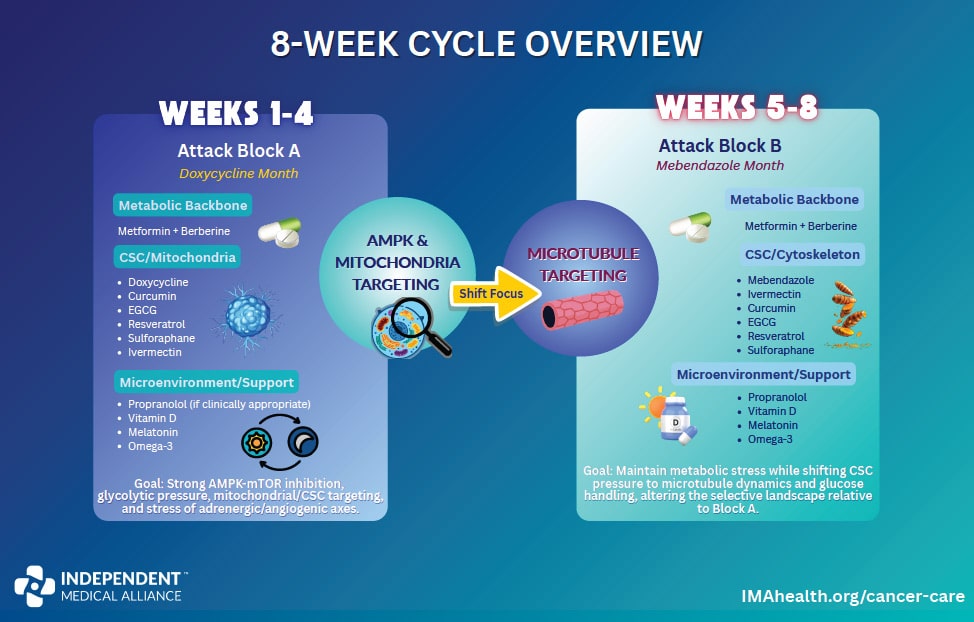
The timing and sequencing matter as much as the drugs themselves.
- Multi-pathway drugs (metformin, berberine, propranolol, and melatonin) are far less prone to resistance because they hit multiple targets at once. They run continuously through both phases of the cycle. Skip a month, and the cancer refuels through that open door.
- Single-pathway drugs (doxycycline and mebendazole) are vulnerable to resistance under sustained pressure. They alternate monthly in an eight-week cycle, applying shifting pressure that keeps the cancer cell metabolically trapped.
All five drugs are inexpensive, widely available, and carry well-established safety profiles. For families already under the financial and emotional weight of a cancer diagnosis, that accessibility matters.
Dr. Cole compared the challenge to the hydra of Greek mythology: cut off one head and two grow back. You have to cauterize each one.
“It’s similar in cancer. We want to cut off certain cancer pathways that are good for the cancer. We want to kill those. And then we want to be able to get the cell back to normal.” — Dr. Ryan Cole
A frontal assault on one pathway just sends the tumor off to the side. The multi-axis approach is the flanking maneuver.
4. Diet, Gut Health, Light, and Stress
Both physicians are clear on this point: dietary change is foundational to cancer care, not a supplement to it.
Cancer cells consume glucose at roughly 16 times the rate of a normal cell. Choking off that fuel source is, in Dr. Marik’s view, as important as any medication a patient will receive. He shared the story of a dermatologist with metastatic breast cancer who had been treated for 10 years. She had seen multiple oncologists and gone through multiple rounds of chemotherapy. Not one of them ever mentioned diet.
“I was the first person that actually explained to her the cancer lives on glucose. You’ve got to change your diet.” — Dr. Paul Marik
This is a pattern Dr. Marik sees repeatedly, and he considers it a fundamental failure of standard cancer care. The metabolic approach calls for:
- A low-carb, whole-food diet
- Intermittent fasting
- Eliminating ultra-processed foods, including juices and sugary drinks
- Glucose restriction as a deliberate therapeutic strategy
IMA has published several guides on this topic, including Nutrition for Cancer Prevention, Cancer Nutrition Guide, and Dietary Interventions in Cancer.
Gut health is equally critical. With 70 to 80 percent of the immune system based in the GI tract, an unhealthy microbiome leads to sluggish immune response no matter how well the drug protocol is designed. Cycling doxycycline monthly, rather than running it continuously, also serves to protect the microbiome from sustained antibiotic pressure.
Morning sunlight sets the circadian clock, triggers melatonin production cycles, and delivers near-infrared light that directly powers mitochondrial function. Most people associate melatonin with sleep, but the intracellular melatonin produced by mitochondria is actually the most powerful antioxidant within the cell. Spending the day indoors under artificial light depletes this system entirely.
“Your body cycles every day. You don’t have high insulin all day, high cortisol all day. When you’re treating something that’s off-cycle, you’re trying to cycle something to match the most beneficial timing of treating human physiology.” — Dr. Ryan Cole
Propranolol, the low-dose beta blocker in the protocol, addresses an often-overlooked factor: stress. At just 20mg twice daily, it blocks adrenergic receptors on tumor cells. Women on propranolol do significantly better with breast cancer. It’s not about sedation. It’s about dampening the stress response that actively fuels tumor growth.

5. Remission Is Not the Finish Line
Getting the good news that a tumor is in remission changes everything for a patient. But it doesn’t mean the fight is over.
Dr. Marik pointed to the experience of Jane McClelland, author of How to Starve Cancer, who treated her own cancer, went into remission, stopped her medications, and then relapsed. Dormant cancer cells can remain in the body for years, potentially reactivating when the metabolic pressure is lifted.
After remission, the intensity of the protocol can be reduced, but some form of maintenance therapy is likely necessary for life. The same principle applies after surgery. As Dr. Marik explained, surgery itself can cause cancer cells to break off and circulate in the bloodstream, potentially seeding metastases. IMA publishes a preoperative protocol specifically designed to reduce that risk.
Every patient is different. Tumor biology, genetics, immune function, diet, and stress all shape the treatment response. That’s why this approach must be guided by a clinician who can monitor progress and adapt the strategy in real time.
“The days are gone where physicians dictate therapy and patients passively accept whatever they’re told. Patients need to take ownership and need to be involved.” — Dr. Paul Marik
For patients whose doctors are unwilling to discuss metabolic or repurposed drug approaches, Dr. Marik’s advice is direct: find a physician who will. The resources to support that conversation are freely available through IMA’s Cancer Resource Hub.
Related Reading
- Monograph: Cancer Care
- New Guide: The Metabolic Trap: Multi-Axis Metabolic Pressure in Cancer Therapy
- New Guide: Cancer Resistance and Interventions to Mitigate Resistance
- Hub: IMA Cancer Resource Hub
- Guide: Nutrition for Cancer Prevention
- Guide: Cancer Nutrition Guide
- Guide: Dietary Interventions in Cancer

