


Approach to the Use of Repurposed Drugs in Patients with Cancer
*Please note: ‘Cancer Care: The Role of Repurposed Drugs and Metabolic Interventions in Treating Cancer,’ and all scientific references, can be found here: imahealth.org/research/cancer-care
The approach to each patient must be individualized based on the type and stage of the tumor, the tumor biology, the patients’ comorbidities and functional status and the patients’ preferences. Many patients may receive repurposed drugs and metabolic therapy as adjunctive therapy to conventional therapy from an oncologist while others may receive repurposed drugs and metabolic therapy alone. There is no ideal regimen; however, our approach is centered on the primary use of ivermectin, mebendazole, doxycycline and curcumin. It should be recognized that a subset of patients appear to either not respond to ivermectin or respond minimally to the initial ivermectin dose, but MAY respond to higher doses. It is essential that multiple cancer stem cell (CSC) pathways are blocked. There are basically two approaches (with a spectrum in between), namely:
- Limited Therapy: Start with a limited number of agents at low doses and increase the dose and the number of agents in patients who don’t This approach is preferred in patients with limited disease or those receiving multiple conventional therapies (esp. breast cancer).
- Aggressive Therapy: Start with a high dosage and number of agents; then cut back slowly in those patients who respond or add additional agents in those who fail to respond adequately. This approach is preferred in patients with metastatic disease or highly aggressive tumors.
Limited Therapy
- Low carbohydrate, Low Glycemic Broccoli sprouts 2x to 3x per week (sulforaphane), brewed green tea (< 4 cups/day)
- Ivermectin 2-0.4 mg/kg/day (0.3 mg/kg/day).
- Doxycycline 50 mg daily taken together with 2 g oral vitamin C (consider cycling after 6 months)
- Vitamin D 10 000 U daily and Vitamin K2 100 ug (monitor 25-OH Vit D and PTH levels)
- Curcumin extract twice daily (high bioavailability). Daily dose of 2 -4 g titrate up to 8 g/day
- Melatonin 20 mg at night (titrate up from 5 mg)
- Resveratrol 500 mg twice a day (high bioavailable)
- Green tea extract (EGCG) twice a day (< 800 mg/day)
Aggressive therapy
- Low Glycemic “ketogenic diet” (add broccoli sprouts 2x to 3x per week).
- Ivermectin 0.4-0.8 mg/kg/day (0.6 mg/kg/day). Increase the dose as tolerated up to 1 mg/kg/day if the response is
- Mebendazole 200 mg daily
- Doxycycline 50 mg daily taken together with 2g oral vitamin C (consider cycling after 6 months)
- Vitamin D 10 000 U daily and Vitamin K2 100 ug (monitor 25-OH Vit d and PTH levels). Titrate to achieve a low normal PTH level (Coimbra Protocol)
- Curcumin extract twice daily (high bioavailability)
- Metformin 500 – 1000 mg twice daily
- Green tea extract (EGCG) twice a day (< 800 mg/day)
- Melatonin 20 mg at night (titrate up from 5 mg)
- Resveratrol 500 mg twice a day (high bioavailable)
- Modified Citrus Pectin (Pectasol 4 g/day; 6 tablets three times a day)
- Sulforaphane (free stabilized sulforaphane extracted from broccoli seeds); dosage varies
- Omega 3 fatty acids 2-4 g/day
- Atorvastatin 40-80 mg daily or simvastatin 40 mg daily (do not use long term or cause a precipitous reduction of LDL due to increased risk of dementia)
- Propranolol 20-40 mg twice daily
- Quercetin 500-1000 mg twice daily
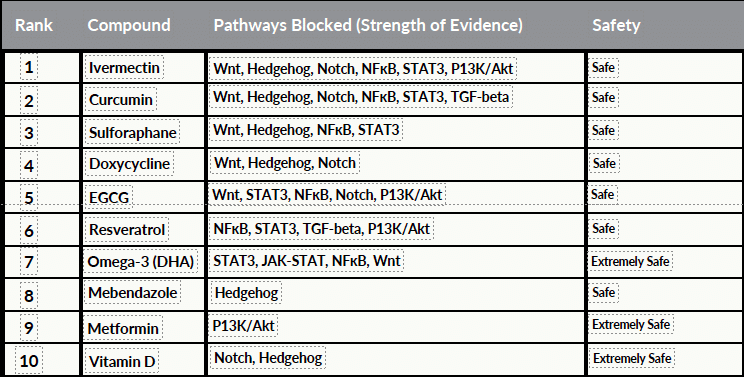
Tables 1 and 2 below were generated using two different Artificial Intelligence (AI) engines, and were then validated and checked. They rank repurposed drugs according to clinical efficacy, Cancer Stem Cell (CSC) pathways blocked, and overall safety.
Table 1. Combining anti-cancer ranking, Stem Cell pathway activity and safety.
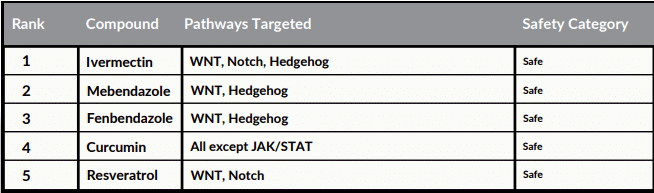
Table 2. The following table ranks the top 10 compounds based on their Cancer Stem Cell (CSC) blocking activity, summarizes their pathway inhibition, and evaluates their safety profile based on therapeutic index and commonly used doses.
The Limited and Aggressive therapeutic approach as outlined above applies to patients with “generic cancers.” Based on limited clinical data and supported by AI (reviewed and validated) we outline below the agents that we believe should be incorporated into the treatment of the most common types of cancer in the “typical cancer” patient. It should be recognized that these protocols are based on an exploratory AI analysis based on limited data as head-to-head studies have not been performed and the algorithms that AI uses are unclear. This information should therefore be used as a guide in formulating patient specific treatment. Furthermore, we believe that these repurposed drug combinations can prevent Stage 1 or Stage 2 cancers from progressing to deadly Stage 4 disease with the goal of inducing a remission.
Prostate Cancer
- Doxycycline (plus vitamin C)
- EGCG
- Ivermectin
- Sulforaphane
- Curcumin
- Metformin
- Modified Citrus Pectin (Pectasol 4 g/day; 6 tablets three times a day)
- Mebendazole
- Resveratrol
- Zinc 15mg (dose < 20mg) for nonmetastatic See caution below*
- Quercetin (synergizes with EGCG)
Colorectal Cancer
- Ivermectin
- Curcumin
- Sulforaphane
- Metformin
- Atorvastatin/simvastatin
- Modified Citrus Pectin
- Resveratrol
- EGCG
Breast Cancer
- Mebendazole
- Ivermectin
- Curcumin
- Doxycycline and vitamin C
- Sulforaphane
- Modified citrus pectin
- Atorvastatin/simvastatin
- Resveratrol
- EGCG
Lung Cancer (small cell)
- Curcumin
- EGCG
- Metformin
- Mebendazole
- Sulforaphane
- Atorvastatin/Simvastatin
- Doxycycline and vitamin C
Lung Cancer (NSCLC)
- Mebendazole
- Ivermectin
- Curcumin
- EGCG
- Metformin
- Sulforaphane
- Atorvastatin/Simvastatin
- Modified citrus pectin
- Doxycycline and vitamin C
Endometrial Cancer (uterine cancer)
- Metformin
- Curcumin
- Ivermectin
- Sulforaphane
- Mebendazole
- ECGC
- Resveratrol
- Atorvastatin
- Modified citrus pectin
Melanoma
- Mebendazole
- Ivermectin
- Doxycycline plus vitamin C
- EGCG
- Metformin
- Sulforaphane
- Modified citrus pectin
Liver Cancer
- Mebendazole
- Ivermectin
- Curcumin
- Doxycycline plus vitamin C
- Sulforaphane
- ECGC
- Metformin
- Modified citrus pectin
- Melatonin
Ovarian Cancer
- Mebendazole
- Curcumin
- Sulforaphane
- Metformin
- Ivermectin
- Atorvastatin/Simvastatin
- Resveratrol
- Doxycycline plus vitamin C
- Modified citrus pectin
Head and Neck Squamous Cancer
- Doxycycline plus vitamin C
- EGCG
- Metformin
- Mebendazole
- Ivermectin
- Curcumin
- Modified citrus pectin
Pancreatic cancer
Pancreatic cancers have significantly worse outcomes than most other types of cancer. Nearly half (49.5%) of metastatic pancreatic cancers spread to the liver and 20.3% to the lungs. The median survival for patients with liver metastases is estimated at less than three months. Unfortunately, many of the repurposed drugs are not active against pancreatic cancer cells. The drugs listed below reportedly have activity against pancreatic cancer cells.; this list is an adaption of the Bigelsen Treatment Protocol.
- Curcumin
- High dose vitamin D3 (Coimbra protocol)
- Doxycycline plus vitamin C 2g (PO)
- Ivermectin (start dose at 1 mg/kg and increase as tolerated)
- Metformin
- Atorvastatin/Simvastatin
- Modified citrus pectin
- High dose IV vitamin C (50- 75g) together with standard chemotherapy (gemcitabine and capecitabine)
- Hydroxychloroquine 200-400 mg day; max dose of 5 mg/kg/day to reduce retinopathy Regular eye exams are recommended to detect early signs of retinal toxicity.
Gastric Cancer
The prognosis for gastric cancer varies significantly based on several factors, including the stage at diagnosis, the location of the tumor, and the patient’s overall health. The prognosis is best for localized cancers, with a 5-year relative survival rate of about 75%. For regional cancers, the rate drops to around 35%.
- Atorvastatin
- Ivermectin
- Curcumin
- Metformin
- Modified citrus pectin
- Resveratrol
Glioblastoma
Glioblastoma continues to be one of the most challenging malignancies to treat, with median survival typically around 12-15 months despite aggressive standard therapies. The concept of drug repurposing offers a promising approach to enhance conventional treatments by targeting resistant cell populations, particularly cancer stem cells that contribute significantly to treatment failure. Several repurposed agents demonstrate synergistic effects with standard GBM treatments. The evidence from various studies indicates that many of these agents work through distinct yet complementary mechanisms that could collectively enhance treatment outcomes. Because GBM is a very aggressive tumor with an exceedingly poor prognosis we would suggest combining all the repurposed drugs listed below together with conventional therapy.
- Curcumin
- Doxycycline plus vitamin C
- Metformin
- Resveratrol
- Melatonin
- Mebendazole
- Sulforaphane
- Ivermectin (See paragraph below for more)
- Atorvastatin/Simvastatin
- Zinc (30mg day)
- EGCG
Despite ivermectin’s limited BBB penetrability, several factors suggest it may still exert immune activity against GBM. These include the inherent disruption of the BBB in GBM tumors, Ivermectin’s systemic immunomodulatory effects, its ability to convert “cold” tumors to “hot “tumors and potential for enhanced delivery through combination approaches. Perhaps most importantly for GBM applications, Ivermectin has shown the capacity to convert “cold” tumors (with little immune infiltration) to “hot” tumors (with significant immune infiltration). This property is particularly relevant to GBM, which is characterized by substantial local immunosuppression and is often considered a “cold” tumor resistant to immunotherapy
Based on available in vitro evidence, the triple combination of modified citrus pectin, PD-1 inhibitors, and ivermectin would likely demonstrate substantial synergistic anti-cancer activity in GBM. While each agent has individual activity or paired synergy, the combined approach addresses multiple complementary pathways that could overcome the complex immunosuppressive mechanisms in GBM. It should be noted that there is no clinical data to support this combination.
Repurposed drugs for patients with established stage 4 metastatic disease.
- Doxycycline (up to 200 mg/day) plus vitamin C
- Ivermectin
- Mebendazole
- Curcumin
- Metformin
- Resveratrol
- ECGC
- Atorvastatin/Simvastatin
Based on the cumulative evidence from preclinical studies and limited clinical data, the likelihood of this combination arresting progression and potentially reversing metastatic cancer would be moderate to substantial. Several factors support this assessment:
- The combination targets multiple hallmarks of cancer simultaneously, including CSC pathways, metastatic processes, and the tumor
- Multiple agents in this combination have demonstrated synergistic effects with conventional chemotherapeutics, potentially enhancing treatment efficacy.
- Several of these compounds preferentially target CSCs, which are implicated in treatment resistance and disease
However, important limitations must be acknowledged. The majority of evidence comes from preclinical studies rather than randomized clinical trials. Stage 4 cancer is highly heterogeneous, and response may vary significantly based on cancer type and individual patient factors. The specific combination of all agents has not been systematically studied for potential interactions
Preventing cancer progression from carcinoma in situ (stage 0 cancer)
- Doxycycline plus vitamin C
- EGCG
- Mebendazole
- Resveratrol
- Ivermectin
- Metformin
- Sulforaphane
- Curcumin
- Modified citrus pectin
Acute Myeloid Leukemia (AML) – Pediatric (no radiation and standard chemo)
AML represents a heterogeneous hematologic malignancy with significant treatment challenges. Even with standard treatments, resistance mechanisms often lead to relapse, with leukemic stem cells playing a crucial role in this process. The JAK/STAT, NF-КB and PI3K/AKT pathways are constitutively activated in AML. Therefore, in addition to standard chemotherapy the following compounds are suggested:
- Doxycycline plus vitamin C
- EGCG
- Mebendazole
- Resveratrol
- Ivermectin
- Metformin
- Sulforaphane
- Curcumin
- Modified citrus pectin
Curcumin and blood thinning: Curcumin has been reported to have blood-thinning properties, which can directly affect the body’s ability to form blood clots. The bleeding risk is heightened when curcumin is combined with certain medications:
- Anticoagulants: Warfarin, heparin, and other blood thinners
- Antiplatelet drugs: Aspirin, clopidogrel (Plavix)
- Non-steroidal anti-inflammatory drugs (NSAIDs)
The increased bleeding risk associated with curcumin can manifest in various ways:
- Easy bruising
- Abnormal bleeding (e.g., nosebleeds, bleeding gums)
- Blood in stool or urine
- Prolonged bleeding times
- Excessive bleeding during surgery
To mitigate the bleeding risk associated with curcumin:
- Discontinue curcumin supplementation at least two weeks prior to any scheduled
- Be cautious when combining curcumin with other herbal supplements that may affect blood clotting, such as garlic, ginkgo biloba, or fish
- Monitor for signs of increased bleeding, such as easy bruising or prolonged bleeding from
Metformin and Berberine
Both of these drugs decrease blood glucose. Therefore, to prevent hypoglycemia, the blood glucose should be monitored when using both drugs simultaneously. Alternatively, reduce the dose of berberine to once daily or metformin to 500 mg twice daily.
Doxycycline and the Microbiome
Doxycycline use appears to have minimal impact on the overall composition and diversity of the gut microbiome:
- No significant differences were observed in bacterial taxonomic alpha diversity or beta diversity between doxycycline users and controls2.
- The normalized bacterial mass of the gut microbiome remained stable after doxycycline
- No consistent differential abundance of bacterial genera was found between baseline and after six months of doxycycline use.
Green Tea (EGCG) and Hepatotoxicity
EGCG is rarely reported to cause liver injury. Risk of toxicity is reduced when dose of EGCG < 800/day, the dose is gradually increased over weeks, and it is taken with food and/or vitamin C. Brewed tea (≤4 cups/day) poses minimal hepatotoxicity risk. Curcumin taken together with EGCG may increase the risk of hepatotoxicity. Curcumin should not be combined with piperine as it is likely to increase the risk of hepatotoxicity. Liver function tests should be monitored regularly in these patients, particularly when initiating therapy. These supplements should be avoided in patients with a history of liver disease or those who are currently on CLL-directed therapy. Furthermore, USP verified supplements are recommended.
*Zinc and Prostate Cancer
Prostate cancer cells exhibit a 70-80% reduction in zinc levels compared to healthy prostate tissue. Low-dose (1–24 mg/day) post-diagnostic zinc supplement has been associated with a lower risk of lethal prostate cancer and all-cause mortality among men with nonmetastatic prostate cancer (stage I-III). Risks and limitations. High dose (> 75mg/day) and prolonged supplementation (10 years) Zinc supplementation increases the risk and aggressiveness of prostate cancer. While zinc shows promise as a therapeutic agent, the dose-dependent biphasic effect necessitates careful clinical management. Current evidence supports cautious low-dose supplementation particularly for early-stage patients, while avoiding high-dose/long-term use.
