
Repurposed drugs are showing real results in cancer care. Learn practical strategies and dosing from Dr. Paul Marik and Dr. Justus Hope in this free guide.

“You have cancer.”
Nobody is ever truly ready to hear those words. In the days that follow, most patients are quickly swept into a program of chemotherapy, radiation, and surgery. It’s an incredibly scary track to be on—and far too often, it feels like you’re on it alone.
But there’s something important every cancer patient should know: you are not limited to just one set of tools. More and more patients are finding hope — and better outcomes — by working with integrative and adjunctive care doctors who combine conventional treatments with safe, science-backed therapies. This collaborative approach not only addresses the cancer itself, but also supports the whole person through the journey.
That’s exactly why Dr. Paul Marik teamed up with Dr. Justus Hope to create one of the most critical cancer treatment guides available on the planet: Approach to Repurposed Drugs in Patients with Cancer. Backed by decades of clinical experience and the latest science, it’s a lifeline for patients and a trusted roadmap for clinicians who want more than the status quo.

💡 Why We Made This Guide
Cancer Care, the monograph by Dr. Paul Marik, is a huge and valuable resource. It pulls together an extraordinary amount of research, including dosage guidance for dozens of repurposed compounds. But because the cancer treatment landscape is always shifting, there was a need for something more agile—something we could update regularly as new information comes to light.
That’s what this guide is: a streamlined companion to Cancer Care. It has already been updated several times and will continue to evolve, making it a true living document. It was designed with both patients and doctors in mind, and it’s best used when those two parties are working together to shape a care plan. This is also one of several companion guides, all of which can be found at our main Cancer Care page or our growing resource page, the Cancer Hub.
As Dr. Marik explains:
“We provide the clinician but also the patient with an overall guide to how to manage these patients.”
📖 What’s Inside the Guide
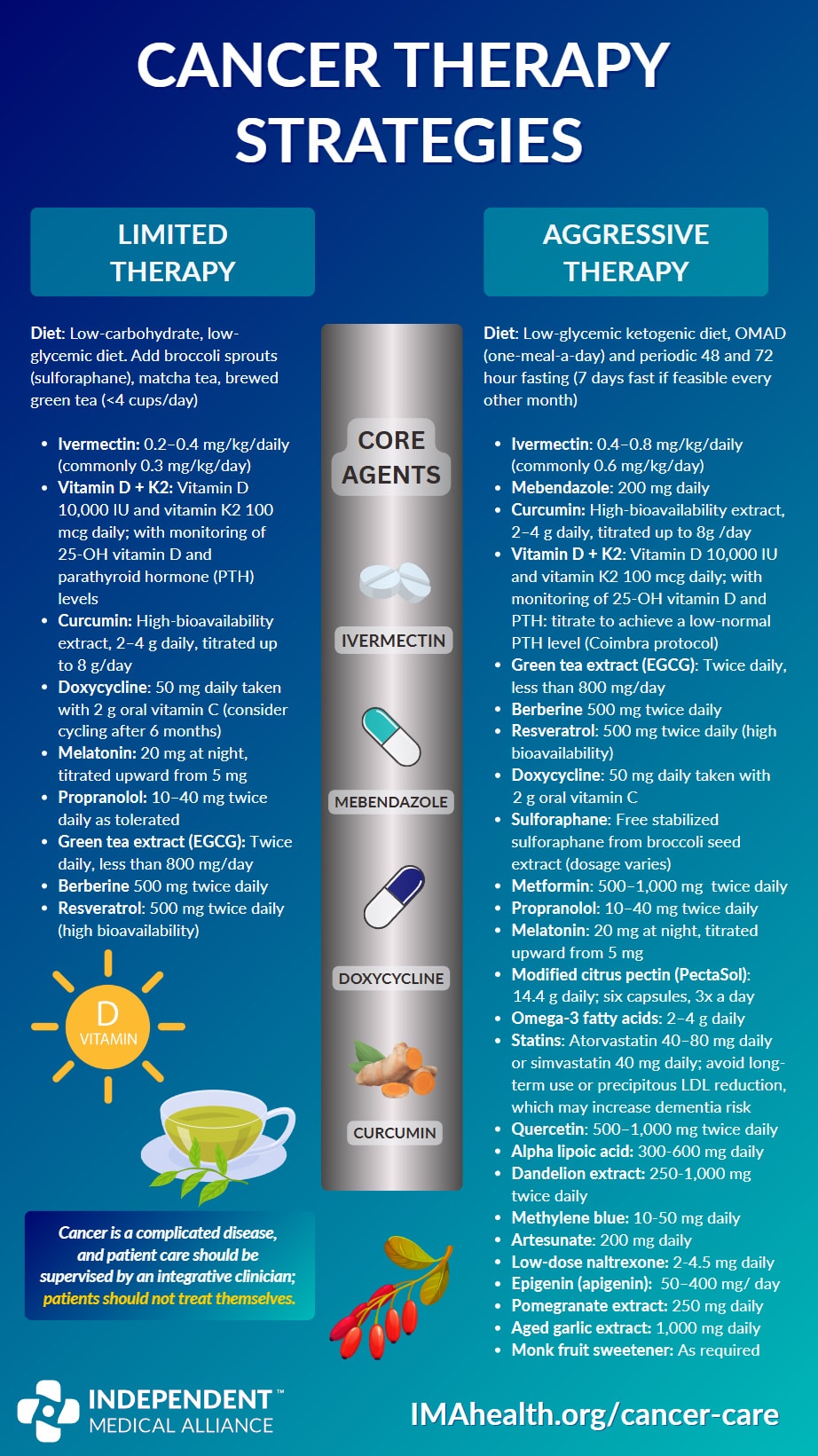
- Two practical tracks for care — a Limited and an Aggressive approach — with core agents and dosing ranges to help you and your clinician choose a starting point.
- Evidence-informed rankings of repurposed compounds, showing which ones block key cancer stem cell (CSC) pathways and how they stack up on safety.
- Cancer-specific protocols for common tumor types (e.g., prostate, breast, colorectal, lung, melanoma, ovarian, endometrial, liver, head & neck, pancreatic, gastric, glioblastoma) plus blood cancers (lymphoma, multiple myeloma, pediatric AML).
- Stage-based guidance for both carcinoma in situ (stage 0) and stage 4 metastatic disease.
- Cautions & interactions you should know (e.g., curcumin with blood thinners, EGCG dose thresholds, zinc nuance in prostate cancer, metformin with berberine).
🎯 Limited vs. Aggressive Approach
For best results, cancer care must be individualized. To make that practical, this guide offers two starting frameworks can be adjusted over time:
- Limited Approach (fewer agents, lower doses, easier to layer alongside conventional therapy) and;
- Aggressive Approach (more agents up front for metastatic or highly aggressive disease, then taper if response is good).
The goal in both is to block multiple cancer stem cell (CSC) pathways while matching intensity to the clinical picture.
The following protocols are drawn directly from the PDF: Approach to Repurposed Drugs in Patients with Cancer.
Last update: January 28, 2026
Limited Therapy Approach
| Intervention | Notes / Dosage |
|---|---|
| Low-carbohydrate, low-glycemic diet | Intermittent fasting/OMAD (one-meal-a-day). Add matcha tea, brewed green tea and/or 4 cups coffee/day. |
| Ivermectin | 0.2–0.4 mg/kg/day (commonly 0.3 mg/kg/day) |
| Vitamin D + K2 | Vitamin D 10,000 IU + K2 100 µg daily; monitor 25-OH D and PTH |
| Curcumin | 1000–2000 mg/day (500–1000 mg twice daily); use highly bioavailable forms (Phytosome, nano-curcumin, CurcuWIN) |
| Melatonin | 20 mg at night, titrate up from 5 mg |
| Propranolol | 10–40 mg twice daily as tolerated |
| Resveratrol | 500 mg twice daily (high bioavailability) |
| Green tea extract (EGCG) | Twice daily (<800 mg/day) |
| Berberine | 500 mg twice daily (hold during multi-day fast) |
Aggressive Therapy Approach
| Intervention | Notes / Dosage |
|---|---|
| Low-glycemic ketogenic diet | OMAD (one-meal-a-day) and periodic 48 and 72 hour fasting (7 days fast if feasible every other month) |
| Ivermectin | 0.4–0.8 mg/kg/day (commonly 0.6 mg/kg/day), with titration up to 1 mg/kg/day if response is poor and drug is well tolerated. Take with food. Reduce dose if experience headaches, dizziness and other neurological signs. |
| Mebendazole | 200 mg daily |
| Curcumin | 1000 – 2000 mg/day (500 -1000 mg twice daily). Use highly bioavailable preparation e.g. Phytosome Curcumin, nano-curcumin or CurcuWIN. |
| Vitamin D + K2 | Vitamin D 10,000 IU daily and vitamin K2 100 mcg; with monitoring of 25-OH vitamin D, Calcium and PTH: titrate to achieve a low-normal PTH level (Coimbra protocol) |
| Green tea extract (EGCG) | Twice daily, less than 800 mg/day |
| Berberine | 500 mg twice daily (monitor glucose if taking metformin) |
| Resveratrol | 500 mg twice daily (high bioavailability) |
| Doxycycline | 100 mg twice daily for 12 weeks (consider repeating after 3 months) or 100 mg daily semi-indefinitely (consider taking a break for a few months) |
| Sulforaphane | Free stabilized sulforaphane from broccoli seed extract (dosage varies) |
| Metformin | 500–1,000 mg twice daily (hold during multi-day fast) |
| Propranolol | 10–40 mg twice daily as tolerated |
| Melatonin | 20 mg at night, titrated upward from 5 mg |
| Modified citrus pectin (PectaSol) | 14.4 g daily; six capsules, three times a day |
| Aged garlic extract | 1000 mg daily |
| Omega-3 fatty acids | 2–4 g daily |
| Statins | Atorvastatin 40–80 mg daily or simvastatin 40 mg daily; avoid long-term use or precipitous LDL reduction, which may increase dementia risk |
| Quercetin | 500–1,000 mg twice daily (stagger dose with Ivermectin) |
| Alpha lipoic acid | 300–600 mg daily |
| Dandelion extract | 250–1000 mg twice daily |
| Methylene blue | 10–50 mg daily + photo-biomodulation (see dosing guidance) |
| Artesunate | 200 mg daily |
| Low-dose naltrexone | 2–4.5 mg daily |
| Epigenin (apigenin) | A plant derived flavonoid, 50–400 mg/day |
| Pomegranate extract | 250 mg daily |
| Monk fruit sweetener | As required |
- Consider high dose IV vitamin C (75 -100 g 2-3 times weekly) together with standard chemotherapy in patients with cancers that express low levels of catalase activity (melanoma, breast, pancreatic, esophageal and lung cancer). Screen for G6PD deficiency.
If you want something you can easily print or share, check out this beautiful infographic our team made:
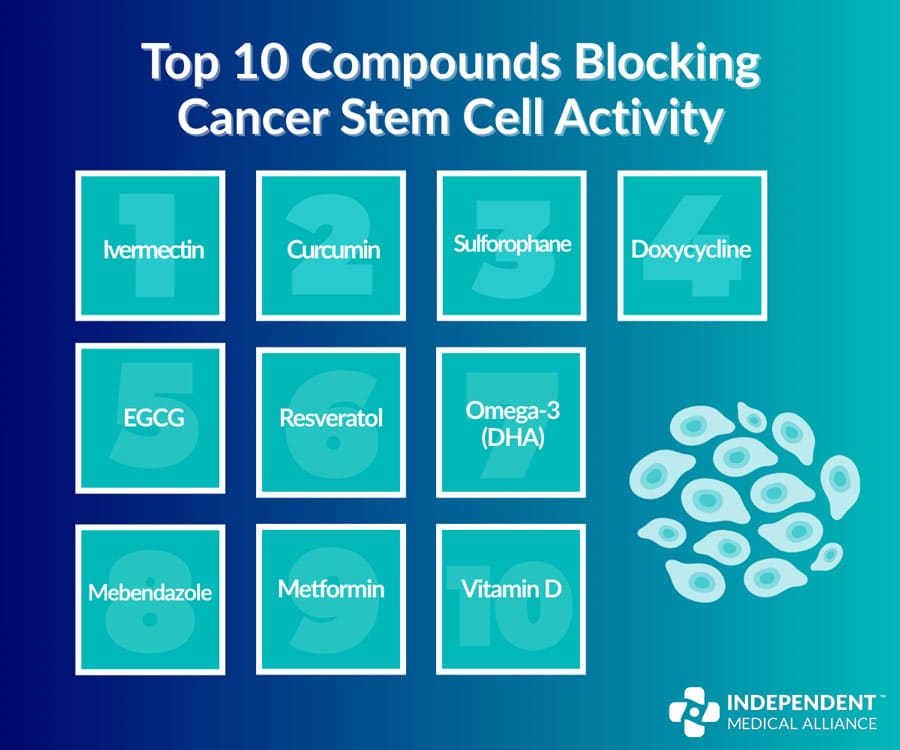
Top 10 Compounds for Cancer Stem Cell (CSC) Blocking Activity
As mentioned above, the goal of using these cancer treating compounds is to target cancer stem cell pathways. Using AI tools, Dr. Marik and Dr. Hope aimed to evaluate both the effectiveness and the safety of the compounds on their list. As you’ll see from the image below, there are a number of safe compounds with evidence to show they work too.
🛠️ Tailoring Repurposed Therapy to Cancer Type
Every patient responds differently, and cancers themselves can behave in unique ways. That’s why this guide doesn’t stop at general strategies—it also highlights cancer-specific approaches so treatment can be better matched to each diagnosis.
The goal remains the same: to block multiple cancer stem cell (CSC) pathways while balancing safety and adaptability. But the details matter, and they shift depending on tumor type, stage, and clinical picture.
Cancers Covered in This Guide
- Prostate
- Breast
- Colorectal
- Lung — Small Cell (SCLC)
- Lung — Non-Small Cell (NSCLC)
- Melanoma
- Ovarian
- Endometrial (uterine)
- Head & Neck squamous cell carcinoma
- Liver (hepatocellular carcinoma)
- Pancreatic*
- Gastric*
- Glioblastoma*
- Lymphoma
- Multiple Myeloma
- Acute Myeloid Leukemia (pediatric)
- Esophageal*
- Sarcomas*
🧭 Special Considerations
It’s worth highlighting that a few cancer types require special attention within this framework. While the principles of repurposed therapy apply broadly, these cancers carry unique challenges and warrant extra consideration:
* Pancreatic Cancer
Pancreatic cancers often have significantly poorer outcomes compared to most other cancers. Metastases to the liver and lungs are common, and median survival for advanced disease remains limited. Many repurposed drugs show little direct activity against pancreatic cancer cells, though certain agents adapted from the Bigelsen Treatment Protocol may provide targeted benefit.
* Gastric Cancer
The prognosis for gastric cancer varies widely depending on stage and patient factors. While localized disease may carry a relatively favorable survival rate, outcomes drop sharply once the cancer becomes regional or metastatic. This variability underscores the importance of tailoring repurposed drug strategies to individual disease stage and context.
* Glioblastoma (GBM)
Glioblastoma remains one of the most aggressive and treatment-resistant cancers, with survival often measured in months. Repurposed drugs may help by targeting resistant cancer stem cells and working synergistically with conventional therapies. Treatment must also account for the blood–brain barrier and the tumor’s strong immunosuppressive environment. Current evidence suggests the best results come when repurposed agents are layered on top of standard therapy, and while certain combination strategies (e.g., modified citrus pectin + PD-1 inhibitors + ivermectin) look promising, robust clinical validation is still lacking.
* Esophageal Squamous Cell Carcinoma (ESCC)
ESCC is highly lethal, and new approaches are urgently needed. Several repurposed drugs appear especially relevant—including azithromycin (weekly, limited course), curcumin, EGCG, vitamin D, quercetin, ivermectin, mebendazole, metformin, resveratrol, and atorvastatin. These agents may offer synergistic benefit alongside conventional treatment and deserve close attention in collaborative patient-clinician decision-making.
* Sarcomas
Sarcomas are rare but often highly aggressive cancers, frequently diagnosed late. Their metabolism is dominated by the Warburg effect, making metabolic interventions attractive. Repurposed agents such as propranolol (especially in angiosarcoma), EGCG, curcumin, vitamin D, mebendazole, and high-dose IV vitamin C are highlighted as potential adjuncts. Because of their biology, sarcomas are a strong case for integrating repurposed therapies with conventional treatment from the outset.
🌅 The Future of Cancer Treatment
Repurposed drugs hold enormous promise for broadening treatment options and giving patients more tools in their fight against cancer. What we’ve shared here is just a starting point—an overview meant to help doctors and patients work together in a more informed way. Every cancer behaves differently, and every patient’s journey is unique, so these combinations are best understood as a framework to guide treatment.
Though alternative treatments can be stigmatized, keep in mind the approach need not be “all or nothing”. Talk to your doctor and work with your patients. Above all, remain hopeful and look forward with bravery.
📚 More Cancer Care Resources
IMA is dedicated to creating and curating vital cancer resources. This mission began with Dr. Marik’s Cancer Care monograph, but since then it has become a focus for many of our contributors. Have a look at these extended cancer resources below:
- Guide: Cancer Nutrition Guide: Support Healing with Food
- Webinar: Journal of Independent Medicine No. 3: Turbo Cancer Research & More
- Webinar: Cancer Care: Research and Insights from the Frontline
- Post: $14 Billion Later, Cancer Is Worse Than Ever. Where Did the Money Go?
- Post: The 10 Deadliest Cancers—and How to Stop Them

