
Host: Dr. Joseph Varon | Guests: Dr. Peter McCullough and Nicolas Hulscher, MPH
One in 31 children in the United States now has autism spectrum disorder. In California, the number is 1 in 12 boys. The prevalence has climbed every year for decades, and the institutions responsible for investigating why have produced no actionable explanation. They have, however, produced a very clear message: stop asking about vaccines.
A new peer-reviewed paper in the Journal of Independent Medicine refuses that framing. “Determinants of Autism Spectrum Disorder” is the first comprehensive review to map every major class of autism risk factor into a single framework, from genetics and parental age to environmental toxicants, gut-brain disruption, and the cumulative childhood vaccine schedule. It draws on 308 references. It reviews 136 vaccine-related studies. And it names what most of the existing literature has been structured to avoid: the full pediatric schedule has never been evaluated for neurodevelopmental safety.
For families who watched a healthy child regress after a round of vaccinations, the paper puts evidence behind what they already know. But it also challenges both sides of a debate that has calcified into false certainty. Those who dismiss vaccines as a factor default to genetics as destiny. Those who focus exclusively on vaccines miss the other seven categories of risk. This paper exists to shatter both misconceptions. Autism likely has many determinants, and studies like this one give parents and physicians the tools to help reverse the trend.
The authors aren’t claiming a single cause. They’ve mapped the determinants, identified the most modifiable one, and laid out exactly what research the field has failed to do.

📖 Read and Download the Full Paper
Determinants of Autism Spectrum Disorder (Journal of Independent Medicine Vol. 2, No. 3, 2026)
Authors: Nicolas Hulscher, John S. Leake, Simon Troupe, Claire Rogers, Kirstin Cosgrove, M. Nathaniel Mead, Breanne Craven, Mila Radetich, Andrew Wakefield and Peter A. McCullough
👉 Visit the Journal of Independent Medicine to create a free account and download the full article.
Meet the Experts

Peter A. McCullough, MD
Internist, cardiologist, and trained epidemiologist; President, McCullough Foundation. One of the most widely published physicians in the country, Dr. McCullough’s recent work spans vaccine injury syndromes, spike protein-related illness, and neuropsychiatric disorders.

Nicolas Hulscher, MPH
Lead author; McCullough Foundation, Dallas, TX. Since 2023, Hulscher has contributed to more than 20 peer-reviewed studies spanning COVID-19 vaccine injury syndromes, H5N1 avian influenza, and autism spectrum disorder.
1. Eight Risk Factors, One Framework
Autism research has spent decades studying risk factors in isolation. This paper treats them as a system. It identifies eight major categories and maps how they intersect in susceptible children:
- Parental age: Risk rises when both parents are over 40. Fathers over 40 face roughly 5.75 times the risk compared to fathers under 30.
- Sibling history: Having a sibling with ASD increases risk by 5 to 10 times.
- Genetic variants: MTHFR polymorphisms affect folate metabolism and DNA methylation, both essential to neurodevelopment.
- Prematurity: Children born before 37 weeks face approximately a 20% risk of autism.
- Environmental toxicants: Pesticides, PFAS, heavy metals, and air pollution all show associations.
- In utero drug exposure: More than 20 drug classes, including anticonvulsants and antipsychotics, are associated with increased risk.
- Gut-brain axis: Children with ASD are at least four times more likely to have gastrointestinal problems. Abnormal microbiome profiles appear in virtually every case studied.
- Childhood vaccination: The authors identify this as one of the most significant modifiable factors, given exposure to up to 81 recommended doses by age 18 under the current CDC schedule.
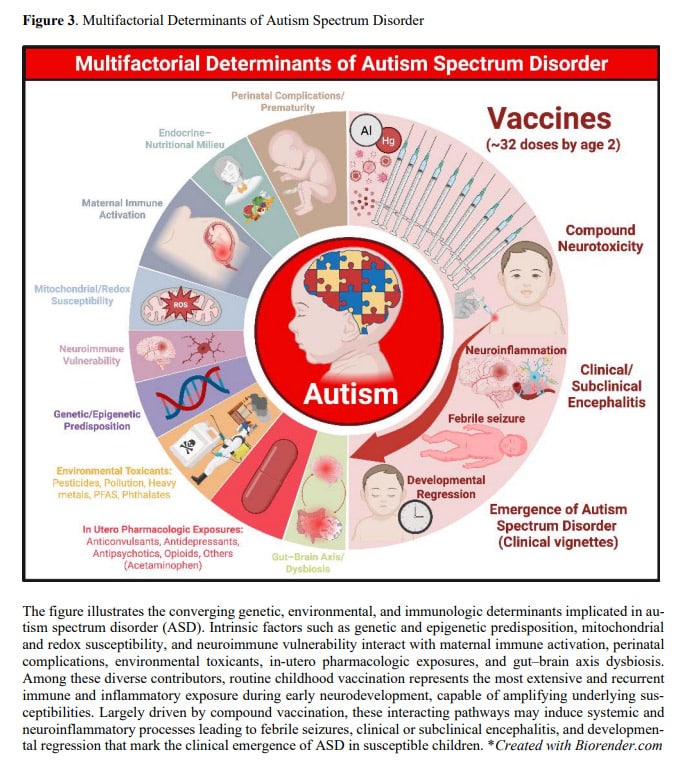
The paper’s central figure maps how these factors converge on shared biological pathways: immune dysregulation, mitochondrial dysfunction, and neuroinflammation. The point is not that any one of these causes autism. The point is that they compound, and the children at highest risk are the ones carrying the most predisposing factors when they enter the heaviest vaccination window.
Building that framework required casting a wide net. The review encompassed 308 references across every domain the authors could identify.
“We searched, scavenged the entire peer-reviewed literature for any possible exposure or genetic polymorphism or really anything that could possibly contribute to autism.” — Nicolas Hulscher
2. Why the Vaccine Schedule Gets Special Attention
The paper reviewed 136 studies examining childhood vaccines or their components. Of those, 107 inferred a possible link to ASD or other neurodevelopmental disorders. Twenty-nine found no association.
That 29-to-107 ratio is striking on its own. But the paper goes further, examining why those 29 found nothing. The pattern is consistent: no genuinely unvaccinated control group. Reliance on registry-based ICD codes without verifying vaccine records or confirming diagnoses through direct examination. Averaged estimates that obscure effects in vulnerable subgroups. Not one employed a non-inferiority framework to evaluate ASD as a safety endpoint.
The 12 studies that did include completely unvaccinated children all found the same thing: lower rates of chronic disease and neuropsychiatric disorders in the unvaccinated group. Every time. The Henry Ford Health System birth cohort, the largest at 18,468 children followed for 10 years, found vaccinated children had 5.53 times higher rates of neurodevelopmental disorders.
Meanwhile, the CDC’s Autism Spectrum Network operates 16 research sites and tracks 25,000 children with autism. According to McCullough, not one of those children has had their vaccine records directly examined.
“Not in a single case has the CDC examined their vaccine records, nor have they examined the other factors that we did in the McCullough Foundation report.” — Dr. Peter McCullough
That’s 25,000 children. Decades of surveillance. And the most basic investigative step, looking at what those children were actually exposed to, has never been taken.
3. Developmental Regression: What Parents See
This is where the science meets the lived experience of thousands of families. A child develops normally through the first year. Language emerges. Social engagement builds. Then, typically in the second year of life, skills disappear. Language drops away. Eye contact stops. The child withdraws.
The paper estimates roughly one-third of autistic children experience some form of developmental regression. Only five published case reports and case series document the pattern in clinical detail. In every one, vaccination was the preceding event. No comparable reports exist for other individual exposures.
McCullough frames what he sees clinically: autism looks like a post-encephalitic syndrome. The biology supports him. Twenty vaccines list brain inflammation in their package inserts. A Swedish study followed 73 children with febrile seizures and found that 41% had neurodevelopmental disorders by age nine or ten.
“Autism, in my clinical view, looks like a post-encephalitic syndrome.” — Dr. Peter McCullough
The paper identifies five biological pathways connecting vaccination to regression, several of which are potentially treatable:
- Immune dysregulation: Vaccine-induced cytokine cascades may trigger or amplify neuroinflammation in susceptible children.
- Mitochondrial dysfunction: The Poling case, published by a Johns Hopkins neurologist whose own daughter regressed at 19 months after a battery of vaccines, documented acquired mitochondrial deficits that were not genetic.
- Oxidative stress: Impaired methylation capacity and depleted glutathione have been measured in children with ASD.
- Neuroinflammation: Postmortem and imaging studies show microglial activation in autistic brains consistent with a post-encephalitic process.
- Cerebral folate deficiency: Antibodies against folate receptors develop in some autistic children. Folinic acid (leucovorin) can address this directly.
These aren’t theoretical mechanisms. They are documented in the children who regressed.
4. What the Paper Doesn’t Claim
The paper uses the word “determinants,” never “cause.” It maps risk factors and their interactions. It does not argue that every case of autism has a single explanation, and it is careful about what the evidence rules out:
- Acetaminophen: A 2.48-million-patient Swedish study (Ahlqvist et al., JAMA 2024) with sibling controls found no independent association. Women who took Tylenol during one pregnancy but not another showed no difference in autism outcomes between siblings.
- Thimerosal as the sole driver: Mercury-based preservatives have declined to near zero in childhood vaccines, yet autism continues to rise.
- Aluminum as a sole determinant: Present in roughly 60% of vaccine doses, but McCullough notes that clinical aluminum neurotoxicity presents differently from autism.
What the paper does conclude is that combination vaccines given during critical neurodevelopmental windows, in children who are already predisposed, represent the most significant modifiable risk factor. The brain develops most rapidly between birth and age four. The current schedule recommends approximately 32 doses in the first two years.
“We don’t use the word cause anywhere in the paper. We use risk factors. A good term to use is determinants.” — Dr. Peter McCullough
The precision matters. “Determinants” means the odds of autism are higher when these factors are present. It’s the language of epidemiology, not advocacy. The paper earns its conclusions by showing its work across 308 references.

5. The Research That Hasn’t Been Done
No study has ever evaluated the cumulative safety of the full pediatric vaccine schedule for neurodevelopmental outcomes through age 9 or 18.
That fact sits at the center of the paper. Hundreds of studies have examined individual vaccines or individual components. None has examined what happens when a child receives all of them, on the schedule, in the combinations and timing the CDC recommends. The absence is not an oversight. It is a choice that has gone unchallenged for decades.
McCullough proposes a path forward: use the existing Henry Ford cohort. Professionally examine every child. Interview the families. Verify the vaccine records. The infrastructure exists. The funding does not, because the institutions that control research funding have treated this question as settled.
Hulscher calls for a large case series documenting the biological pathway to regression in hundreds of children. The last published case series was in 2007. Almost 20 years of silence on the most clinically detailed form of evidence available.
Nineteen days after this paper’s press release, the CDC updated its public stance: the connection between vaccines and autism “has not been ruled out.” The research community now has a peer-reviewed framework, a clear set of evidence gaps, and a public health agency that has acknowledged what families have been saying for a generation.
“If we continue the track we’re on, in 2050 about half of boys in California will be autistic. We’ve got to stop it. We’ve identified the risk factors. Now’s the time for the research community to act.” — Nicolas Hulscher
Related Reading
- Peer-Reviewed Study: Determinants of Autism Spectrum Disorder
- Journal: Journal of Independent Medicine
- Webinar: Autism Affects 1 in 31: One Doctor’s Search for Answers
- Post: New Study Asks: Could Vaccine-Induced Viral Reactivation Trigger Autism?
- Webinar: What’s Driving the Exponential Rise in Autism? And Why Listening to Parents is So Important.
- Webinar: Autism, Vaccines, and the Search for Truth
- Webinar: Are 72 Vaccines Too Many? A Legal Case Against the CDC
