
Patients with elevated sodium levels face significantly higher mortality and longer hospital stays. New research published in the Journal of Independent Medicine quantifies the risk and points toward prevention.
For critical care teams, sodium isn’t just another number on the chart. It’s a signal. According to this new research, it may be much more consequential than previously understood.
A new study published in the Journal of Independent Medicine analyzed data from over 150,000 hospitalizations and found that patients with acute respiratory failure who develop hypernatremia—elevated sodium levels—face nearly 50% higher mortality and hospital stays that more than double. The study was co-authored by an incredible team, including IMA/FLCCC co-founders Dr. Joseph Varon and Dr. Jose Iglesias, as well as IMA Director of Research Matthew Halma and newcomer Edgar Selemi.
“Having a high sodium level was an independent risk factor for people to die or to have worsening complications from respiratory failure,” says Dr. Joseph Varon, IMA President and study author. “This is actually something extremely important, especially for those of us who continue to work in critical care.”
📖 Read and Download the Full Paper
Impact of Acquired Hypernatremia in the ICU on Mortality in Patients with Acute Respiratory Failure: A Retrospective Analysis from the NIS Database (JIM Vol. 2, No. 1, 2026) Authors: Edgar Selemi, Jose Iglesias, Matthew Halma, Joseph Varon
👉 Visit the Journal of Independent Medicine to create a free account and download the full article.
About the Study
The research team analyzed the National Inpatient Sample (NIS) database from 2018–2021—one of the largest publicly available all-payer inpatient databases in the United States. Out of 153,840 patients hospitalized with acute respiratory failure (median age 64, 56% male), half were identified with hypernatremia.
Key findings:
- Mortality: 28.2% in hypernatremic patients vs. 18.9% without (OR=1.522, p<0.001)
- Length of stay: 11 days vs. 5 days
- Illness severity: Significantly higher in the hypernatremia group (OR=1.273)
- Routine discharge: Less likely for hypernatremic patients (OR=0.814)
Certain comorbidities amplified the risk dramatically:
| Comorbidity | Mortality Odds Ratio |
|---|---|
| Diabetes insipidus | 11.664 |
| Dementia | 2.192 |
| Acute kidney injury | 1.630 |
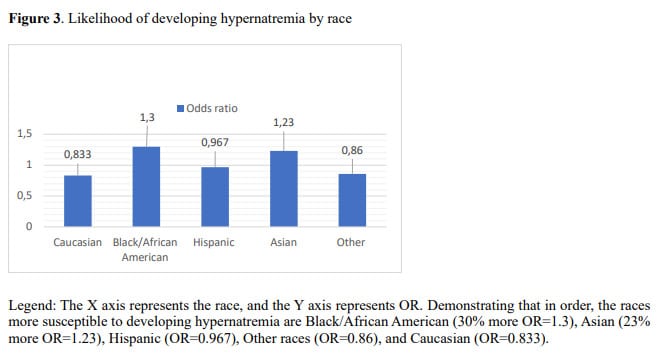
The study also identified racial differences and varying clinical courses that the authors flag as areas requiring further investigation.
Under the Microscope: Why Sodium Levels Matter
For patients and families watching a loved one in the ICU, understanding what clinicians are monitoring can feel overwhelming. But sodium is one of the more straightforward markers to grasp—and one worth paying attention to.
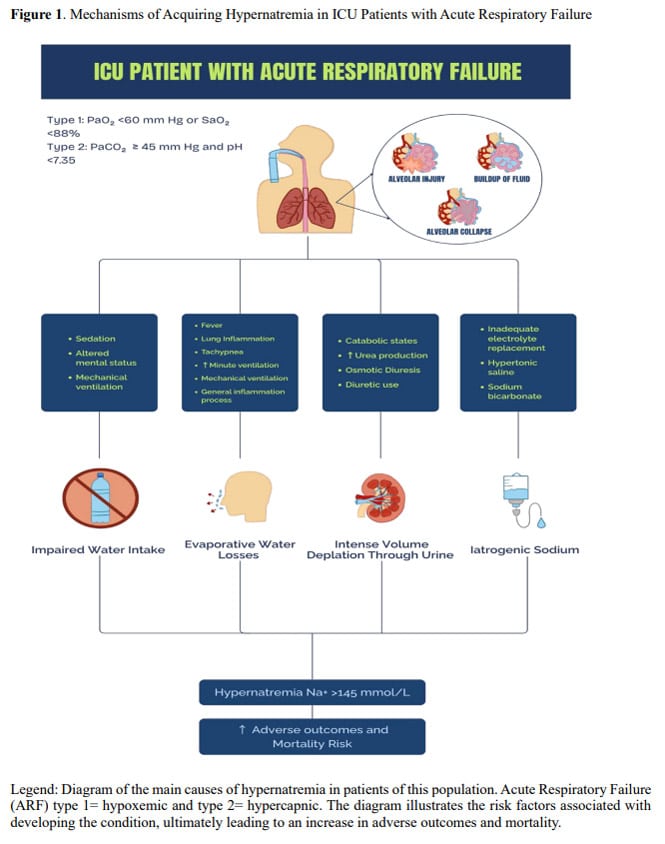
Sodium helps regulate fluid balance, nerve function, and muscle contractions. In the ICU, where patients may be sedated, on ventilators, or unable to communicate thirst, sodium levels can drift upward without obvious warning signs. Causes range from dehydration and medication effects to impaired kidney function.
What this study makes clear is that hypernatremia isn’t just a lab abnormality to note—it’s a clinical red flag. Patients who develop it face worse outcomes across the board: higher mortality, longer ventilator dependence, and reduced chances of going home with a routine discharge.
The good news? Sodium levels are part of routine blood work. The opportunity for early detection already exists. What this research adds is the evidence base to act on it more aggressively.
A Window for Prevention
The authors are direct about the clinical implications:
“Routine ICU monitoring of blood gases facilitates the detection and the opportunity to create a proper management plan to improve the outcomes… Proper management of hypernatremia is needed to avoid the worst outcomes and should be personalized depending on each specific patient.”
For ICU teams, this means treating hypernatremia not as a secondary finding but as an independent target for intervention. For patients and families, it’s a reminder that asking questions (What are the sodium levels? Are they trending up?) is both reasonable and potentially of critical importance.
Back to the Bedside
This study reflects the kind of work that brought IMA’s founding physicians together in the first place: the care of critically ill patients.
“The Independent Medical Alliance continues to do research in the areas that started this organization,” Dr. Varon notes, “which was the care of critically ill patients.”
Before COVID made headlines, IMA’s core team—including study author Dr. Varon and fellow co-founder Dr. Paul Marik—were intensivists developing protocols for sepsis and other ICU challenges. This hypernatremia study is a return to those roots: practical, data-driven research aimed at improving survival for some of the sickest patients in the hospital.
It’s also a fitting way to open Volume 2 of the Journal of Independent Medicine. After a strong first year, the journal continues to publish research that matters to clinicians and patients alike. This is work that might not find a home in pharma-funded publications, but that addresses real gaps in care. Naturally, the Journal exists to provide a platform for medical research that saves lives with no strings attached.
Explore More
This article is featured in Volume 2, Issue 1 of the Journal of Independent Medicine. Stay tuned for more highlights from this issue coming soon!
These resources are free to download—but not free to create. Our medical journal, and every system of technology and review that powers it, requires significant time and resources to build and maintain. Please support our mission to continue sharing evidence-backed medical research with the world by donating today.

