
Dr. Dalgleish’s full interview, captured at the 2026 World Council for Health Better Way Conference in Rhode Island.
At the World Council for Health’s 2026 Better Way Conference, IMA Senior Fellow Dr. Angus Dalgleish did something too few oncologists are willing to do: he laid out, in plain terms, what he has been seeing in his cancer patients since the COVID booster rollout. Within days, on June 3, he delivered the same case to Senator Ron Johnson’s Permanent Subcommittee on Investigations in a hearing titled “Plausible Mechanisms of COVID-19 Injections Causing Cancer and Attacks on Scientific Publications.”
Dalgleish is an Emeritus Professor of Oncology at City St. George’s, University of London, with decades of experience in cancer immunology, HIV research, and vaccine development. He is not speculating. He is reporting what he sees in his clinic, explaining the biology behind it, and asking why the medical establishment won’t connect the dots.
👉 Watch the full Senate hearing: “Plausible Mechanisms of COVID-19 Injections Causing Cancer and Attacks on Scientific Publications”
1. What He’s Seeing
The pattern first appeared in early 2021. Melanoma patients who had been stable for years, some for over a decade, started relapsing. Dalgleish checked their histories. All had recently received COVID booster vaccines. He had seen late relapses before, typically after prolonged immune-suppressing stress: divorce, bereavement, chronic illness. These patients had none of that. What they had in common was a recent booster.
It goes well beyond melanoma. Colorectal cancers that once presented early enough for surgery are now showing up at stage 4 with extensive liver and lung involvement.
“Only last week I had three different people present with stage 4 colorectal cancer with sizeable disease in the liver and lungs. That was extremely unusual. And I was the only doctor who’d seen them, they’d seen dozens and dozens of doctors, who said, ‘Can you give me your vaccine history?’” — Dr. Angus Dalgleish
Cancer incidence had been climbing for decades, driven by processed food, chronic inflammation, and environmental factors. But since the booster rollout, Dalgleish says, the trajectory has steepened: patients are younger, and their cancers are more aggressive. Data from Japan supports the pattern: a peer-reviewed study found that age-adjusted cancer mortality rates increased significantly after the third mRNA vaccine dose. The medical establishment rejects the term “turbo cancer.” Dalgleish points out the phenomenon already has an accepted name in immunotherapy: hyperprogression.
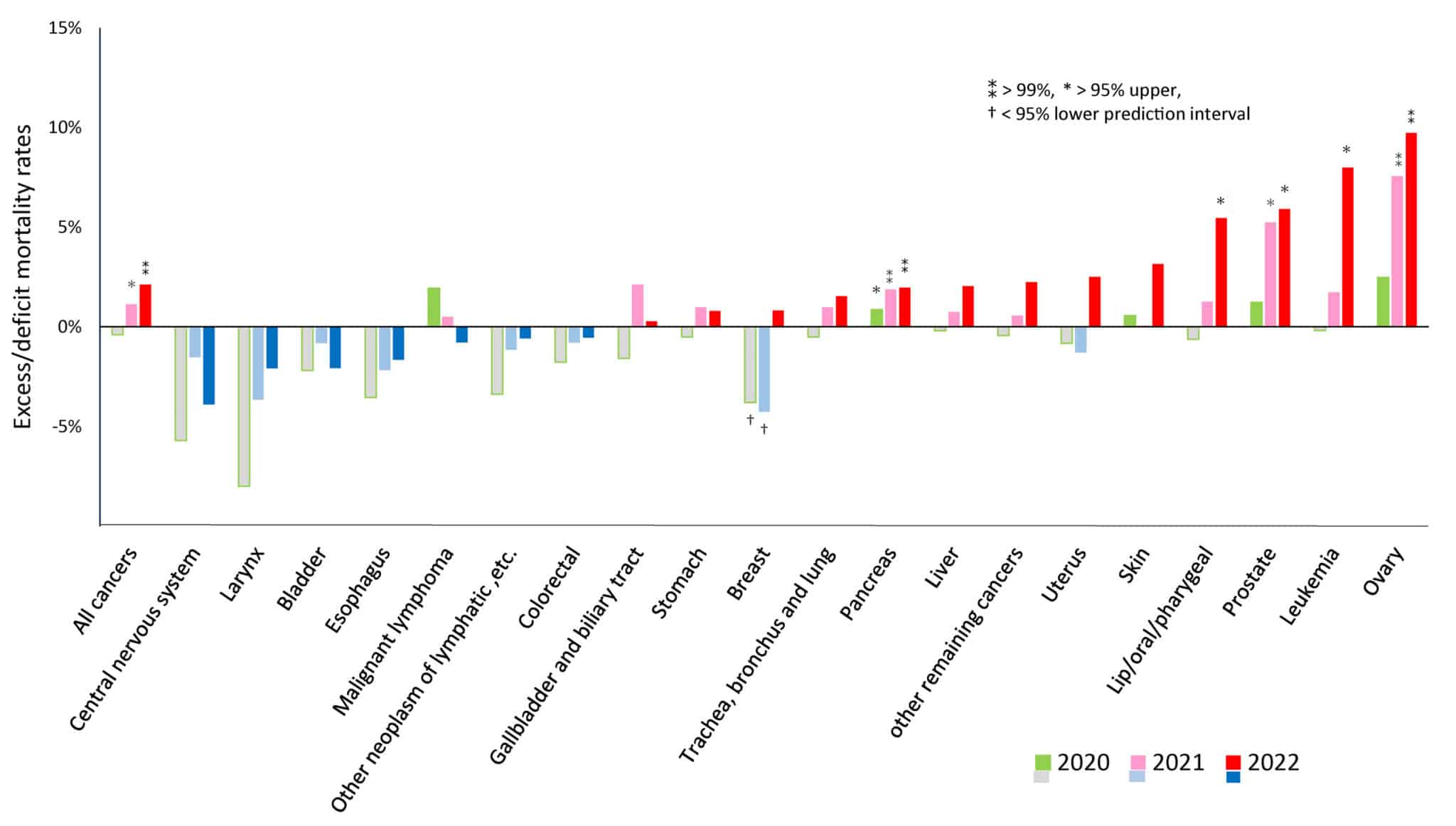
Figure 3: Excess mortality for each cancer type during the pandemic in 2020, 2021, and 2022. Excess mortality = (observed AMR − predicted AMR) / predicted AMR * 100 (%). Source: Increased Age-Adjusted Cancer Mortality After the Third mRNA-Lipid Nanoparticle Vaccine Dose During the COVID-19 Pandemic in Japan (Cureus, 2024)
2. Why He Says It’s the Boosters
Dalgleish doesn’t stop at clinical observation. He walks through the biological mechanisms, each documented in published research, that explain how repeated COVID vaccination could compromise the immune system’s ability to control cancer:
- T-cell exhaustion: A Spanish study demonstrated T-cell suppression in cancer patients after the third COVID vaccine dose. Without functional T-cell surveillance, dormant cancers can escape immune control.
- IgG class switch: Repeated vaccination triggers a shift from effector antibodies (IgG subtypes 1 and 3) to a tolerization antibody (subtype 4), the same class physicians try to induce in transplant patients so they don’t reject a new organ. As Dalgleish puts it: the immune system stops fighting and starts accepting.
- Random genomic integration: Stabilized mRNA integrates into the genome at random, meaning it can land next to an oncogene and switch it on, or next to a tumor suppressor gene and switch it off.
- Manufacturing contamination: Dalgleish describes SV40 promoter sequences and excess DNA levels in vaccine batches, calling the quality control “absolutely diabolical.”
“You cannot control messenger RNA. If you stabilize it, which you have to do to use it as a gene therapy, because that’s what it is, RNA integrates at random. You cannot tell it where to integrate.” — Dr. Angus Dalgleish
3. Why It’s Not Being Heard
When Dalgleish raised these concerns with health authorities, the response was consistent: you’re the only one. He has since learned that dozens of senior clinicians and scientists were told the same thing, individually, at the same time. It is a pattern designed to keep dissenting voices isolated.
He compares it to the UK Post Office scandal, where hundreds of postmasters were accused of theft after a faulty computer system produced false discrepancies. Each was told they were alone. They weren’t.
The media has followed the same script. Dalgleish points to a widely read Daily Mail feature that listed every conceivable driver of rising cancer rates, from processed food to alcohol to obesity, except COVID vaccines. That kind of omission does not happen by accident. It mirrors the broader suppression pattern documented in Senator Johnson’s Unmasked investigation into how Biden-era health officials handled vaccine safety signals.
“This is not quackery. This is not exaggeration. This is a steam train coming down the tracks, and you must stop the vaccines now.” — Dr. Angus Dalgleish
4. What He Says Must Change
Dalgleish’s prescription is direct: stop the COVID booster program, halt mRNA vaccines for infectious disease use, and begin addressing the damage already done.
But his argument goes further than the vaccines. The standard oncology paradigm has always been to kill the cancer and ignore the patient. Dalgleish advocates the opposite: fix the foundation first. His own clinical work with vitamin D, low-dose naltrexone, and repurposed drugs has improved outcomes, but these tools remain locked out of mainstream protocols because no pharmaceutical company stands to profit from them. For patients navigating a cancer diagnosis, that matters.
At the June 3 Senate hearing, Dalgleish testified alongside researchers from Brown University and Tufts University who presented a systematic review of 69 studies examining plausible mechanisms linking COVID vaccines to cancer. The evidence base is growing. What Dalgleish is asking for is simple: that other clinicians and researchers share what they are seeing, before the window to act closes.
“If you think it’s bad now, it’s going to be so much worse in the future. There’s still a window to do something about it.” — Dr. Angus Dalgleish
Related Reading
- Post: Cancer in the Post-COVID Era
- Post: Debrief from Down Under: The State of Censorship in Australia
- Hub: Cancer Resource Hub
- Post: COVID-19 Vaccine Injury: 3 Underlying Mechanisms Mainstream Medicine Still Misses
- Post: Senate Hearing Exposes Study Showing Vaccinated Children Have 2.5x Higher Rates of Chronic Illness
- Webinar: HHS and mRNA: Children, Pregnancy, and What’s Next

